G6PD Deficiency
Key points
- G6PD (glucose-6-phosphate dehydrogenase) enzyme deficiency makes red blood cells prone to hemolysis when exposed to an oxidative stressor such as infection, certain drugs, or fava beans. G6PD screening must be done for those at risk before prescribing primaquine and tafenoquine (e.g., for malaria).
- Globally, G6PD deficiency is the most common enzyme defect, affecting approximately 500 million people.
- All children and youth of African, Asian, Mediterranean and Middle Eastern descent should be considered for G6PD deficiency screening upon arriving in Canada, particularly if they had persistent jaundice as newborns.
- During and shortly after a hemolytic event, the G6PD assay may be falsely normal secondary to reticulocytosis. In such cases, a repeat examination several weeks later may be necessary.
G6PD deficiency
G6PD (glucose-6-phosphate dehydrogenase) is an enzyme that protects red blood cells from injury. G6PD deficiency makes red blood cells prone to hemolysis when exposed to an oxidative stressor, such as infection, certain drugs (see Table 1), or fava beans. Some children with G6PD deficiency present with neonatal jaundice, but many are asymptomatic and can remain undiagnosed until hemolysis is triggered, causing hyperbilirubinemia and sometimes anemia.
Symptomatic episodes are generally self-limited, but may include jaundice, hemoglobinuria, pallor, fatigue, fever, abdominal pain, diarrhea and occasional vomiting. Occasionally, however, the drop in hemoglobin can be severe and require a blood transfusion.
More chronic complications are rare, though it has been noted that individuals with undiagnosed G6PD deficiency often face delayed diagnoses and subsequent complications in conditions such as diabetes, since their HbA1C levels may be falsely lowered.
Globally, glucose-6-phosphate dehydrogenase (G6PD) deficiency is the most common enzyme defect, affecting approximately 500 million people and mainly in African, Asian, Middle Eastern, and Mediterranean populations (see Figure 1). G6PD deficiency primarily affects males because the gene that encodes G6PD resides on the X chromosome. Rarely, females can be affected through homozygosity for G6PD deficiency, or heterozygous females can be affected if their other X chromosome is inactivated.
G6PD variants can be classified into variants that indicate risk of hemolysis. Class A variants are associated with chronic hemolytic anemia, while Class B variants are associated with a risk of hemolysis, while Class C variants are not associated with hemolysis.[1]
Figure 1: Global severity risk of G6PD deficiency (2012)
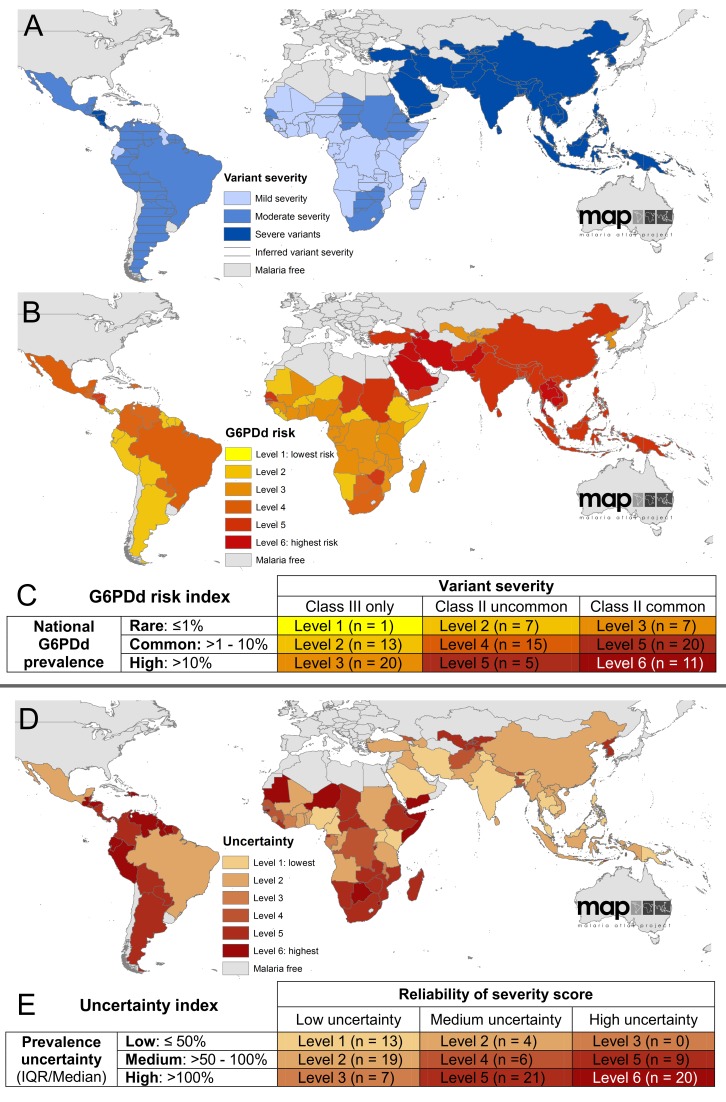
Source: Howes RE, Piel FB, Patil AP, Nyangiri OA, Gething PW, Dewi M, et al. (2012) G6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based Map. PLoS Med 9(11): e1001339. https://doi.org/10.1371/journal.pmed.1001339
Diagnosis
Diagnosis of G6PD deficiency is done through a blood test to measure the level of G6PD enzyme. It is important to note that during and shortly after a hemolytic event, the G6PD assay may be falsely normal secondary to reticulocytosis. In such cases, a repeat level several weeks later may be necessary. G6PD assays can also appear falsely normal following a blood transfusion, and a repeat level should be sent three to four months after the transfusion if needed.
Triggers
All children and youth of African, Asian, Mediterranean and Middle Eastern descent should be considered for G6PD deficiency screening upon arriving in Canada, particularly if they had persistent jaundice as newborns.
Primaquine, a malaria drug prescribed for 14 days to prevent relapse of Plasmodium vivax and P. ovale (for hypnozoite eradication or “radical cure”) is an oxidative trigger. Additionally, tafenoquine is a newer anti-malarial that is being used in many areas of the world and is also an oxidative trigger. Of note, it cannot be discontinued after initiation since it only requires a single dose. Therefore, G6PD screening must be done for individuals at risk before prescribing primaquine and tafenoquine.[1]
Many other drugs can trigger hemolytic crisis, including sulfa antibiotics and antipyretics (see Table 1). Other triggers include infections, naphthalene (mothballs), and fava beans.
Although patients should be cautioned to avoid these triggers when possible, response to triggers varies among patients and is not always consistent.
Table 1: Safety of oxidizing agents in patients who have G6PD deficiency*
|
Generally unsafe for all variants |
Generally safe for class B variants |
|
Acetanilide Furazolidone Methylene blue Nalidixic acid Naphthalene Nitrofurantoin Phenazopyridine Phenylhydrazine Primaquine Sulfacetamide Sulfamethoxazole Sulfanilamide Sulfapyridine Tafenoquine Thiazosulfone Toluidine blue Trinitrotoluene |
Acetaminophen Ascorbic acid Aspirin Chloramphenicol Chloroquine Colchicine Diphenhydramine Isoniazid Phenacetin Phenylbutazone Phenytoin Probenecid Procainamide Pyrimethamine Quinidine Quinine Streptomycin Sulfamethoxypyridazine Sulfisoxazole Trimethoprim Tripelennamine Vitamin K |
*Bold text indicates the agents that are used most commonly in children and youth or are widely used in general.
†Class B variant: G6PD enzyme deficiency <45%, associated with neonatal jaundice; acute hemolytic anemia triggered by medicines, fava beans, or infection; no chronic hemolytic anemia[2]
Source: Adapted from Jeng M and Vichinksy E. Hematologic problems in immigrants from Southeast Asia. Hematol Oncol Clin N Am 2004;18(6):405-22. With permission.
Information for families
- The Hospital for Sick Children. About Kids’ Health. G6PD Deficiency
References
- Luzzatto L, Bancone G, Dugué PA, Jiang W, Minucci A, Nannelli C, Pfeffer D, Prchal J, Sirdah M, Sodeinde O, Vulliamy T, Wanachiwanawin W, Cunningham J, Bosman A. New WHO classification of genetic variants causing G6PD deficiency. Bull World Health Organ. 2024 Aug 1;102(8):615-617.
- Ramiah Vickers, Sarah Elsea. P498: G6PD deficiency: A 'hidden' diagnosis beyond pharmacogenomics. Genetics in Medicine Open 2026;4(1):103990.
Reviewer(s)
Meghna Dua, MD
Andrea Hunter, MD
Last updated: June, 2026